
What if bloating isn’t just from last night’s pizza?
If it shows up most days, wakes you at night, or comes with weight change, blood in your stool, fever, or vomiting, it’s more than annoying.
Here I list the warning signs that point to something serious, simple first steps you can try at home, what to track for your clinician, and the red flags that need same-day evaluation.
If you’re worried, this will help you decide whether to book an appointment or get emergency care.
Clear Signs Persistent Bloating Needs Medical Evaluation

Bloating after a big meal or too many salty snacks? Totally normal. But when it starts showing up three or four times a week, you’re not dealing with occasional puffiness anymore. That’s chronic, and it’s worth talking to someone about. A one-off episode, even if it’s uncomfortable, usually doesn’t mean much. When the same pattern keeps coming back for weeks and you can’t point to an obvious reason, your body’s trying to tell you something.
Frequency isn’t the only thing that matters. There’s a difference between mild bloating that’s gone by morning and the kind that makes your waistband hurt or keeps you from eating normally. Pay attention to quick changes. A belly that swells noticeably over a few days, pain that wakes you up at night, bloating paired with weight you didn’t try to lose. Even five or ten pounds dropping off over a couple weeks alongside bloating is a red flag. Blood in your stool, a fever that won’t quit, vomiting that outlasts a stomach bug, or not being able to pass gas or stool at all? That’s not “annoying” anymore. That needs attention now.
Some situations can’t wait for an appointment next week. If any of these show up, get evaluated same day or head to the ER:
- Sudden, severe abdominal pain that stops you cold
- Abdominal swelling that gets worse over hours, not days
- Can’t pass stool or gas for more than 24 hours
- Persistent vomiting with abdominal pain and distention
- Fever above 101°F with bloating and belly tenderness
- Fainting, dizziness, or confusion alongside abdominal swelling
Common Causes Behind Persistent Bloating That Won’t Go Away
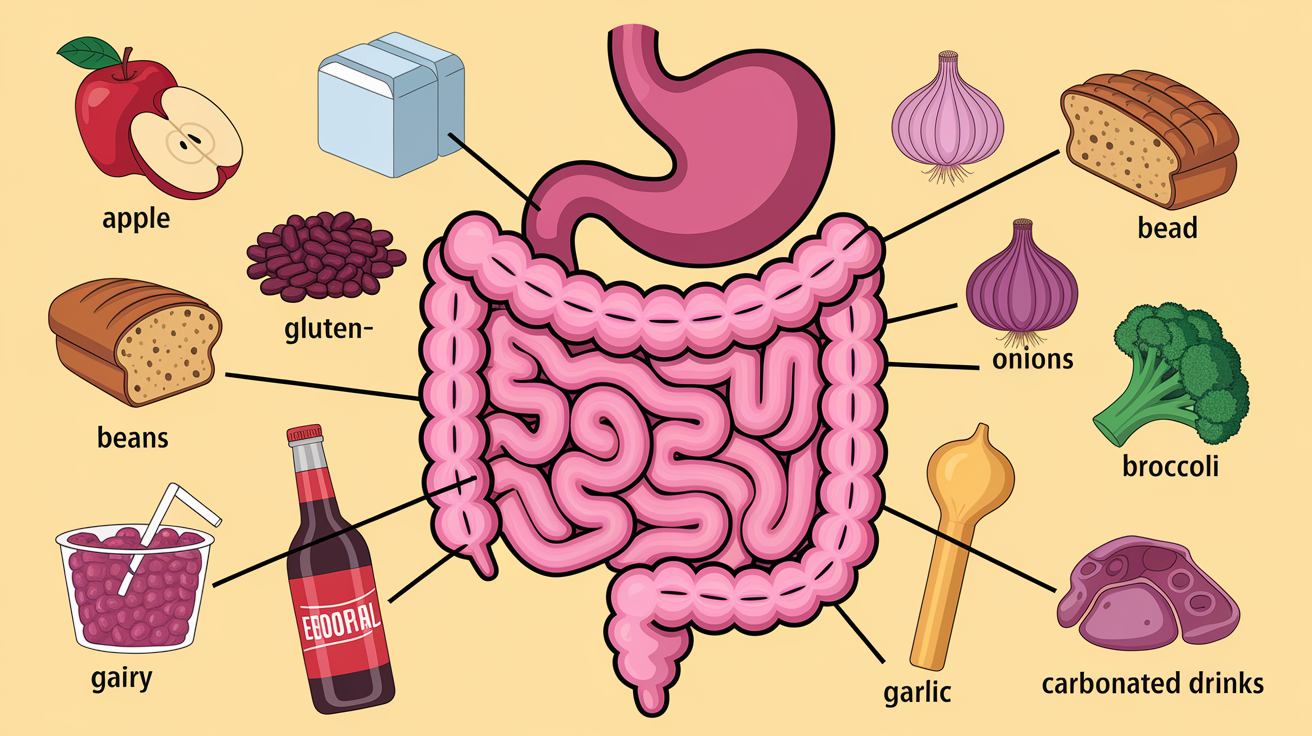
Diet’s usually the first place to look. Eating too much at once stretches your stomach and intestines, cranking up gas production. Eating too fast means you’re swallowing air and not chewing food properly, both of which slow everything down and trap gas. Even healthy foods can cause trouble when they’re loaded with certain carbs (FODMAPs) your small intestine can’t absorb well. Bacteria in your colon ferment what’s left over, making gas and pulling water into your bowel. Both create that tight, uncomfortable feeling.
Food intolerances are common culprits. Can’t break down lactose? That sugar in milk, cheese, and yogurt gets left for bacteria to handle instead. The result is bloating, cramping, and loose stools. Gluten sensitivity and celiac disease do similar things when wheat, barley, or rye are involved. Carbonated drinks pump gas straight into your digestive tract. And sitting around all day slows everything down. Muscles that don’t move don’t help food and gas move through.
Medical causes start mattering when tweaking your diet doesn’t help. IBS messes with the coordinated muscle contractions that push food along, creating trapped gas and alternating between constipation and diarrhea. Gastroparesis (delayed stomach emptying) leaves food sitting too long, often linked to nerve damage and more common in women. Inflammatory bowel disease damages intestinal tissue and creates narrow spots that trap gas. Constipation itself goes hand in hand with bloating. Some people don’t realize they’re backed up until bloating becomes a daily thing.
High-FODMAP foods that trigger bloating over and over:
- Apples, pears, watermelon, stone fruits
- Broccoli, cauliflower, Brussels sprouts, cabbage, onions, garlic
- Beans, lentils, chickpeas
- Wheat-based breads, pasta, cereals
- Milk, soft cheeses, ice cream
Why Certain Symptom Patterns Signal Higher-Risk Conditions
Bloating by itself is usually mechanical or food-related. But when it shows up with other stuff, the combination changes what doctors start looking for. Unintentional weight loss with bloating suggests your gut isn’t absorbing nutrients right, or something’s burning calories faster than you’re replacing them. You see that pattern in celiac disease, inflammatory bowel disease, pancreatic insufficiency, and certain cancers. Blood in the stool means damage somewhere along the GI tract. Could be inflammation, ulcers, polyps, tumors. Fever means infection or active inflammation that might be in one spot (abscess, diverticulitis) or systemic (IBD flare). Steady abdominal swelling that doesn’t change with meals points to fluid buildup (ascites), organ enlargement, or obstruction, not just gas.
These patterns matter because they point to structural problems, not just functional ones. Functional bloating (IBS, swallowed air) is annoying but it’s not damaging anything. Structural or inflammatory processes destroy tissue, risk complications like perforation or bleeding, and need specific treatment. Vomiting that won’t stop suggests something’s blocking normal transit, either mechanically or functionally. New constipation or diarrhea in someone over 50, especially with bloating and bleeding, raises concern for colorectal cancer. The symptom combo narrows down what to test for and speeds up the whole process.
| Symptom Pattern | What It Suggests | Why It Matters Clinically |
|---|---|---|
| Bloating + unintentional weight loss | Malabsorption, inflammation, or tumor | Indicates tissue damage or metabolic drain requiring urgent workup |
| Bloating + blood in stool | Mucosal injury, polyps, IBD, cancer | Bleeding from GI tract requires visualization and biopsy |
| Bloating + fever + abdominal tenderness | Infection, abscess, or severe inflammation | Risk of perforation, sepsis, or need for surgical intervention |
| Progressive distention not relieved by bowel movement | Obstruction, ascites, or organ enlargement | Suggests mechanical or fluid issue rather than gas; imaging essential |
Comparing Abdominal Bloating vs True Abdominal Swelling

Bloating and distention sound alike, but the difference matters. Bloating is that full, pressured feeling, usually from gas trapped in your intestines. It fluctuates. Worse after meals, better in the morning, relieved when you pass gas or have a bowel movement. You can press into a bloated belly and it still feels soft, even if it’s tight. Distention is visible, measurable swelling that doesn’t just come and go with eating. Your clothes fit differently every day, your belly looks rounder in pictures, and the swelling might feel firm or tense instead of squishy.
True abdominal distention raises concern for ascites (fluid in your abdominal cavity), often tied to liver disease, heart failure, or cancer. Could also signal bowel obstruction, where stool and gas back up behind a blockage, or masses (tumors, enlarged organs) pushing outward. Timing helps tell them apart. Bloating that’s gone by morning or after fasting is almost always gas. Distention that’s still there when you wake up, gets worse steadily over days or weeks, or appears lopsided (one side more than the other) needs imaging and clinical evaluation to rule out structural issues.
Medical Evaluation Steps Doctors Use for Persistent Bloating
Evaluation starts with your story. How long has bloating lasted, how often does it happen, what makes it worse or better, what else is going on? Your doctor will ask about bowel habits, diet (especially dairy, wheat, high-fiber foods, carbonated drinks), medications, surgeries, family history of GI disease, any recent travel or antibiotic use. Physical exam includes pressing on your belly to check for tenderness, masses, or fluid, listening with a stethoscope for bowel sounds, sometimes a rectal exam to check for blood or obstruction.
Blood tests look for inflammation (elevated white count, C-reactive protein), anemia (which can point to bleeding or malabsorption), celiac markers (tissue transglutaminase antibodies), thyroid function, liver or pancreatic enzyme levels. Stool tests can catch infections, blood (even tiny amounts), fat malabsorption, or inflammation markers like fecal calprotectin. Imaging (abdominal X-ray, ultrasound, CT scan) shows structural stuff: masses, fluid, bowel dilation, thickened intestinal walls, signs of obstruction. Upper endoscopy lets them look directly at your esophagus, stomach, and upper small intestine. Biopsies can diagnose celiac disease, gastritis, or ulcers. Colonoscopy checks the colon for polyps, inflammation, strictures, or cancer.
What each test looks for:
- Blood work: Inflammation, anemia, celiac antibodies, thyroid or liver dysfunction
- Stool tests: Infection, bleeding, fat malabsorption, inflammatory markers
- Breath tests: Lactose intolerance, small intestinal bacterial overgrowth (SIBO)
- Abdominal imaging (X-ray, ultrasound, CT): Masses, fluid (ascites), bowel obstruction, organ enlargement
- Endoscopy and colonoscopy: Direct view of mucosal lining, biopsies for celiac, IBD, or cancer
When Persistent Bloating Requires Specialist Referral

Your primary care doctor handles the first round, but certain patterns push you toward a specialist. If blood work, stool tests, and imaging point to inflammatory bowel disease, celiac disease, or suspected cancer, a gastroenterologist takes over. GI specialists do endoscopy and colonoscopy, interpret breath tests, manage complex motility disorders, and guide treatment for IBS, SIBO, and chronic constipation. If bloating shows up with pelvic pain, irregular periods, or family history of ovarian cancer, a gynecologist might order pelvic ultrasound or CA-125 blood work to rule out ovarian masses or fluid.
Endocrinologists step in when hormonal stuff like hypothyroidism or PCOS might be contributing. Some bloating tied to anxiety, trauma history, or stress-driven gut hypersensitivity benefits from integrated care that includes a psychologist or psychiatrist trained in gut-brain interaction. Referrals happen faster when red-flag symptoms show up, when initial testing finds something abnormal, or when bloating won’t quit despite reasonable diet and lifestyle changes.
Symptoms that usually prompt specialist referral:
- Blood in stool or positive fecal occult blood test
- Unintentional weight loss of more than 5% over a few weeks
- Imaging showing masses, thickened bowel, strictures, or ascites
- Persistent symptoms after eight weeks of diet tweaks and over-the-counter measures
Benign vs Concerning Patterns in Long-Term Bloating

Benign bloating follows a rhythm you can predict, tied to food, timing, and lifestyle. Shows up after meals heavy in FODMAPs, dairy, or carbonated drinks. Gets better overnight or after a bowel movement. You notice it gets worse when you’re stressed, sitting around, or eating too fast, and it fades when you slow down, move more, or adjust what you’re eating. This kind of bloating is uncomfortable but stable. It doesn’t escalate, doesn’t wake you at night, doesn’t come with weight loss, fever, or bleeding.
Concerning patterns break those rules. Bloating that wakes you from sleep, sticks around despite fasting, or gets steadily worse over weeks isn’t just gas. Constant distention unrelated to meals suggests fluid, a mass, or obstruction. Bloating that starts suddenly in someone over 50 with no prior GI issues, especially with new constipation or blood, is a red flag for colorectal cancer. Nighttime symptoms (pain or bloating that disrupts sleep) often point to inflammatory or structural processes rather than functional stuff. When the pattern stops making sense, when removing obvious triggers doesn’t help and the bloating feels different from anything you’ve dealt with before, get evaluated.
How to Track Persistent Bloating Before a Doctor Visit

Tracking turns vague complaints into useful information. Start a simple log: date, time of day, what you ate in the previous six hours, severity (rate it 0 to 10), how long it lasted, what made it better or worse. Note bowel movements (frequency, consistency using the Bristol Stool Chart helps), any blood or mucus. Track your weight weekly. Even small unexplained losses matter. Write down other symptoms that show up with bloating: cramping, nausea, heartburn, diarrhea, constipation, fatigue, changes in appetite.
Look for patterns. Does bloating spike after dairy, gluten, beans, or carbonated drinks? Does it show up at the same time each day, or cluster around your menstrual cycle? Does it improve with walking, get worse when you’re stressed, or follow antibiotic use? Bring this log to your appointment. It speeds diagnosis by showing your doctor exactly what’s happening and helps them figure out which tests to order first. If you’re on medications (especially antibiotics, NSAIDs, or supplements), list those too. Some drugs mess with gut motility or microbiome balance.
Questions to ask your doctor:
- What are the most likely causes of my bloating pattern based on what you’re seeing?
- Which tests do you recommend first, and what will each one tell us?
- Are there diet changes I should try while we wait for test results?
- How long should I expect before we have a clearer answer?
- What symptoms would mean I need to come back sooner or go to the ER?
- If initial tests are normal, what’s next?
Self-Care Steps While Awaiting Medical Evaluation

While you’re waiting for appointments or test results, safe adjustments can help reduce symptoms. Try eating smaller, more frequent meals instead of three big ones. This reduces the stretch on your stomach and intestines. Chew thoroughly and eat slowly to cut down on swallowed air. Drop carbonated beverages for two weeks and see if bloating improves. The gas from soda and sparkling water is immediate and measurable. If you suspect lactose intolerance, remove dairy for a week. If bloating drops, try lactose-free versions or take lactase enzyme tablets (like Lactaid) before dairy meals.
Gentle movement helps. A 10- to 15-minute walk after meals encourages gut motility and can relieve trapped gas. Probiotics (especially strains like Bifidobacterium and Lactobacillus) might improve bloating in IBS, though results vary. Start with a single-strain product and give it at least two weeks. Adjust fiber carefully. If you’re constipated, slowly increasing soluble fiber (oats, psyllium, ground flax) can help, but adding too much too fast makes bloating worse. If you’re already eating high fiber and still bloated, pulling back slightly might bring relief. A short trial of a low-FODMAP diet (guided by a clear list or app) can clarify whether fermentable carbs are the problem, but don’t stay restrictive long-term without professional guidance.
Simple adjustments worth trying:
- Remove carbonated drinks and chewing gum for two weeks
- Eat slowly, chew thoroughly, avoid talking while eating
- Test eliminating dairy or gluten for one week to identify triggers
- Walk for 10 minutes after meals to encourage motility
- Keep a food and symptom diary to spot patterns
Life-Threatening Bloating Presentations Requiring Immediate Emergency Care

Most bloating isn’t an emergency. But a few scenarios demand immediate action. Sudden severe abdominal pain that makes you double over, especially if your belly becomes rigid or you can’t find a comfortable position, might signal perforation, volvulus (twisted bowel), or ruptured organ. Rapidly worsening distention over hours (not the gradual bloating that builds over days) can mean bowel obstruction or internal bleeding. If you also feel lightheaded, your heart’s racing, or you’re sweating and pale, those are signs of shock. Go to the ER.
Difficulty breathing paired with abdominal swelling suggests either severe distention pushing up on your diaphragm or fluid buildup (ascites) from heart or liver failure. Fainting or near-fainting alongside bloating points to blood loss, severe dehydration, or a cardiovascular event. Vomiting that looks like coffee grounds or has bright red blood, or black tarry stools, means active GI bleeding. These situations go beyond “persistent bloating.” They’re acute, life-threatening, and minutes matter.
Urgent danger signs requiring immediate emergency evaluation:
- Rigid, board-like abdomen with severe pain
- Rapidly progressive distention over a few hours, not days
- Vomiting blood (bright red or coffee-ground appearance)
- Black, tarry stools or large amounts of bright red rectal bleeding
- Lightheadedness, fainting, rapid heart rate, or confusion with abdominal symptoms
- Severe difficulty breathing due to abdominal pressure
Final Words
If your belly feels different or keeps swelling more than 3–4 times a week, this post walked you through what to watch and why.
We covered common everyday causes, the red flags that need prompt care (weight loss, blood in stool, fever, sudden severe pain), how doctors evaluate persistent bloating, and safe steps to try now.
Keep a short log of timing, triggers, and severity so you can decide clearly when to see a doctor for persistent bloating.
Small changes and good notes often point to a simple fix — you’ve got this.
FAQ
Q: When should I be concerned about constant bloating or if my bloat won’t go away?
A: You should be concerned about constant bloating or bloat that won’t go away when it happens more than 3–4 times per week, lasts several weeks, or comes with weight loss, blood in stool, fever, severe pain, vomiting, or progressive swelling.
Q: What are the 5 F’s of abdominal distension?
A: The 5 F’s of abdominal distension are fat (extra body fat), fluid (ascites), flatus (gas), feces (constipation), and fetus (pregnancy), each a common reason the belly looks enlarged.
Q: Can you have 10 lbs of bloat?
A: You can carry roughly up to 10 pounds of bloat from trapped gas, fluid, stool, or recent meals; this feels like sudden weight but usually fluctuates and often eases with diet changes or treatment.
Comments are closed