
Do you spend eight hours in bed and still wake up like you barely slept?
That feeling has a name: non-restorative sleep, which means the hours are there but the repair work isn’t.
It happens when deep slow-wave sleep and REM (the dreaming stage) get chopped up by tiny wake-ups, breathing pauses, pain, stress, or caffeine.
This post will show what morning fog and heavy limbs usually mean, simple changes that often help, what to track before you see a clinician, and when to get checked.
Okay, here’s the simple version.
Understanding Why Non‑Restorative Sleep Leads to Morning Exhaustion

Non‑restorative sleep means you’ve been in bed long enough (usually seven to nine hours), but you wake up feeling like you barely slept. It’s not about the hours. It’s about whether those hours actually did anything for you. When your sleep gets interrupted or fragmented, even in ways you don’t notice, you miss the deeper stages that restore physical energy, lock in memories, and keep your mood steady.
The problem usually comes down to micro‑awakenings during the stages that matter most. Deep slow‑wave sleep is when your body repairs tissue, strengthens immunity, and clears waste from your brain. REM sleep is when your mind processes emotions and consolidates what you learned. If something keeps pulling you out of these stages (noise, breathing pauses, restless legs, stress arousal, an uncomfortable mattress), you cycle back to lighter sleep without finishing the repair work.
Waking during deep sleep triggers what researchers call sleep inertia. That heavy, groggy feeling that can last fifteen minutes or a full hour. Your brain is still half asleep, which is why you might feel disoriented, slow to process anything, or unable to remember simple things right after your alarm. For some people, that fog never really lifts.
Signs your sleep isn’t actually restoring you:
- You feel tired within an hour or two of waking, even after a full night in bed.
- Morning brain fog that persists past your first coffee.
- Can’t get out of bed despite multiple alarms.
- Persistent low energy, irritability, or the sense you “never quite woke up.”
Key Signs Your Sleep Isn’t Restoring Your Energy

There’s a difference between waking up tired once in a while and waking up exhausted almost every day despite doing everything “right.” Non‑restorative sleep is that second pattern. It’s persistent. Frustrating. And it starts affecting how you move through your day.
Daytime symptoms go beyond just feeling sleepy. You might notice slower thinking, trouble remembering details, needing to reread the same sentence three times. Your mood shifts more easily. Irritability, impatience, or a flat feeling that’s hard to shake. Some people describe blank staring episodes or brief moments where they zone out completely (called microsleep). These lapses can happen during meetings, while reading, even while driving. They’re a red flag that your brain is trying to grab rest wherever it can.
Common signs your sleep quality is the problem:
- Daytime drowsiness that hits hardest during passive activities. Sitting in a car, watching a screen, listening to someone talk.
- Morning headaches that ease as the day goes on but return the next morning.
- Difficulty concentrating or holding information in your working memory, even on familiar tasks.
- Increased reliance on caffeine or other stimulants just to feel functional.
- Mood changes like irritability, low frustration tolerance, feeling emotionally flat.
- Microsleep episodes where you briefly lose awareness or stare blankly without realizing it.
Why Non‑Restorative Sleep Happens: Core Sleep Cycle + Sleep Architecture Disruptions
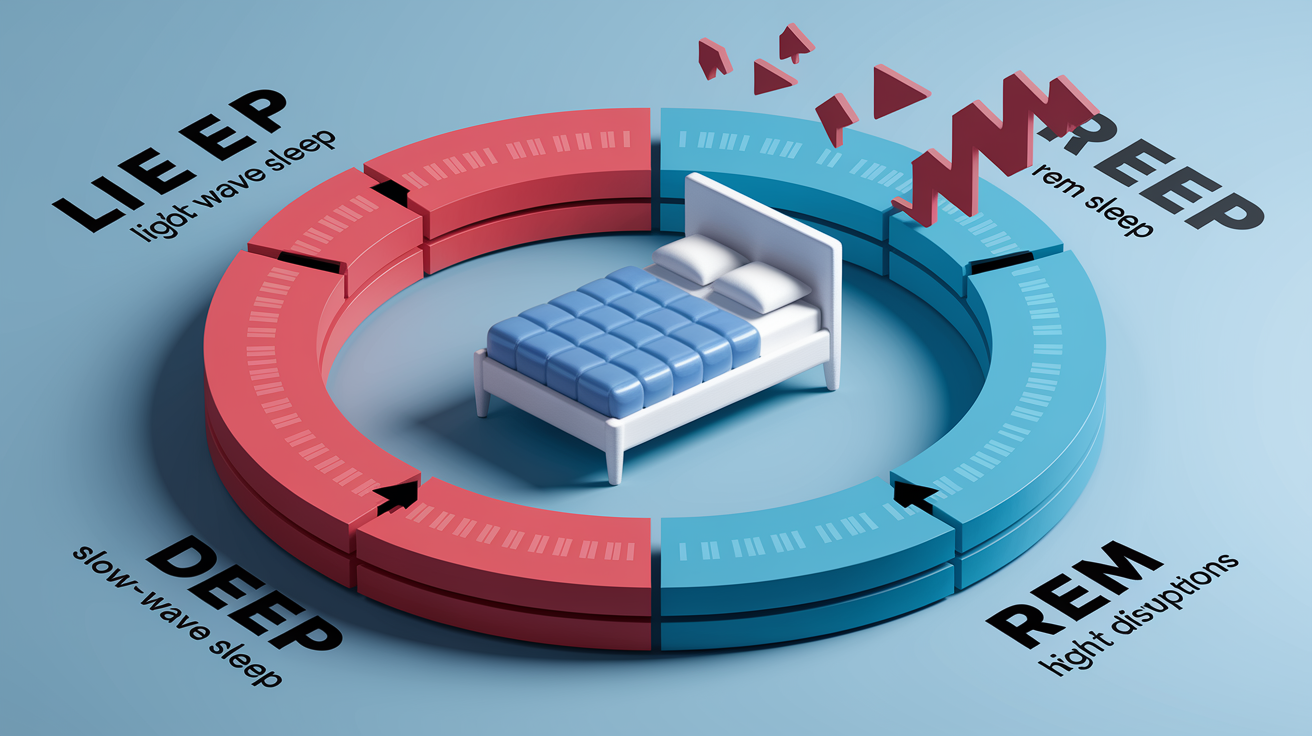
Healthy sleep isn’t one long, unbroken stretch. It’s made up of repeating cycles that move through light sleep, deep slow‑wave sleep, and REM sleep. Each cycle lasts roughly ninety minutes. Deep sleep is when your body does its heaviest lifting: repairing muscle tissue, regulating hormones, strengthening immune function, clearing out waste products that build up in the brain. REM sleep is lighter but just as critical. It’s when your brain processes emotions, organizes memory, makes sense of what happened during the day.
When something interrupts these cycles (stress hormones keeping you in lighter stages, brief awakenings from noise or discomfort, breathing pauses that trigger a partial arousal), you lose continuity. You might cycle back to light sleep before you’ve had enough time in deep or REM. Those lost minutes add up. Over days and weeks, the deficit shows up as persistent fatigue, slower reaction times, mood shifts, and that feeling of being mentally underwater even though you technically “slept.”
The tricky part? Many of these interruptions are invisible. You might not remember waking up, but your brain registered the disruption and pulled you out of restorative sleep anyway. This is why people can spend eight hours in bed and still wake up feeling like they got four. The clock says you slept. Your nervous system says otherwise.
Major Medical and Sleep Disorders Linked to Morning Exhaustion
Obstructive Sleep Apnea
Obstructive sleep apnea happens when the airway repeatedly collapses during sleep, cutting off breathing for ten seconds or longer. Each time that happens, your brain has to pull you partway awake to restart breathing. Sometimes dozens or even hundreds of times per night. You usually don’t remember these events, but they fragment your sleep and keep you from staying in the deeper, restorative stages. Common signs include loud snoring, gasping or choking sounds, waking with a dry mouth or sore throat, morning headaches that fade as the day goes on.
Insomnia Disorder
Chronic insomnia is defined as difficulty falling asleep, staying asleep, or waking too early at least three nights per week for three months or longer, with noticeable daytime consequences. Even when you do fall asleep, the quality is often poor. Your mind stays partially alert, you cycle through lighter stages, you wake feeling like you barely rested. Insomnia can be driven by stress, anxiety, depression, irregular schedules, or conditioned arousal where your bed becomes associated with frustration instead of rest.
Restless Legs Syndrome / Periodic Limb Movements
Restless legs syndrome creates an uncomfortable urge to move your legs, especially at night when you’re trying to settle down. Periodic limb movement disorder involves repetitive jerking or twitching of the legs during sleep. Both conditions can pull you out of deep sleep repeatedly, even if you’re not fully aware it’s happening. People often describe feeling restless all night or waking up with tangled sheets and sore legs, but no clear memory of what interrupted their rest.
Fibromyalgia + Chronic Pain Conditions
Fibromyalgia and other chronic pain syndromes often come with poor sleep quality. Not just because pain makes it hard to get comfortable, but because pain signals can prevent the brain from entering and maintaining deep sleep. Studies show that people with fibromyalgia spend less time in slow‑wave sleep and experience more micro‑arousals, creating a cycle where poor sleep worsens pain sensitivity, and worsened pain further disrupts sleep.
Warning signs pointing to a medical cause:
- Loud snoring, gasping, or witnessed pauses in breathing during sleep.
- Strong urge to move your legs at night, worse when lying down.
- Waking with a racing heart, shortness of breath, or chest discomfort.
- Persistent daytime sleepiness despite spending enough time in bed.
- Morning stiffness, widespread pain, or headaches that improve as the day goes on.
Lifestyle, Behavioral, and Environmental Causes of Unrefreshing Sleep

Even without a diagnosed sleep disorder, daily habits and your sleep environment can quietly chip away at restorative sleep. An inconsistent schedule (going to bed and waking at different times each day, or sleeping in on weekends to “catch up”) confuses your internal clock and makes it harder to fall into deep sleep when you want to. Shift work and jet lag have the same effect, pulling your circadian rhythm out of alignment with your actual sleep window.
Caffeine and alcohol are common culprits. Caffeine taken after mid‑afternoon can still be in your system at bedtime, keeping you in lighter sleep stages even if you manage to fall asleep. Alcohol might make you drowsy initially, but it fragments sleep later in the night, reduces REM sleep, and can worsen breathing issues if you’re prone to snoring or apnea. Mental overload (ruminating on work stress, relationship tension, major life changes) keeps your nervous system revved up, making it hard to drop into the calm state needed for deep sleep.
Your bedroom matters more than most people realize. Clutter, ambient noise, too much light, a mattress that creates pressure points, or a room that’s too warm can all trigger brief awakenings or keep you cycling in lighter sleep. Your body needs to drop its core temperature slightly to enter and stay in deep sleep, so a cool, dark, quiet space supports that process.
| Factor | Impact on Restoration | Typical Warning Sign |
|---|---|---|
| Irregular sleep schedule | Disrupts circadian rhythm; reduces deep sleep consistency | Trouble falling asleep at your target bedtime; variable wake times |
| Late caffeine (after 2 PM) | Blocks adenosine receptors; keeps you in lighter stages | Falling asleep but waking frequently; feeling wired but tired |
| Alcohol before bed | Sedates initially but fragments sleep; reduces REM | Waking in the second half of the night; vivid or disturbing dreams |
| High stress or mental overload | Elevates cortisol and arousal; prevents deep sleep entry | Racing thoughts at bedtime; waking feeling tense or unrested |
| Uncomfortable bedroom environment | Triggers micro‑awakenings from noise, light, heat, or pressure points | Tossing and turning; waking with stiffness or soreness |
Diagnostic Tools for Persistent Morning Exhaustion

When morning exhaustion persists despite reasonable efforts to improve sleep habits, a formal evaluation can help pinpoint what’s disrupting your rest. A clinical sleep evaluation typically starts with a detailed interview about your sleep schedule, nighttime symptoms like snoring or leg movements, daytime functioning, medications, caffeine and alcohol use, and any medical or mental health conditions. You might be asked to keep a sleep diary for one to two weeks, tracking what time you go to bed, how long it takes to fall asleep, how many times you wake, and how you feel the next day.
Questionnaires like the Epworth Sleepiness Scale measure daytime sleepiness by asking how likely you are to doze off in different situations. Sitting and reading, watching TV, riding in a car, sitting quietly after lunch. A score above ten often suggests a sleep disorder worth investigating. If breathing issues, movement disorders, or unexplained daytime sleepiness are suspected, your clinician may recommend overnight testing.
Common diagnostic tools used to evaluate non‑restorative sleep:
- Polysomnography (overnight sleep study): Records brain waves, eye movements, muscle activity, heart rate, breathing patterns, and oxygen levels to detect apnea, limb movements, and disruptions in sleep stages.
- Home sleep apnea test: A simplified version that measures breathing and oxygen during sleep, used when obstructive sleep apnea is the primary concern.
- Actigraphy (wearable tracking): A watch‑like device worn for one to two weeks that tracks rest‑activity patterns to assess circadian rhythm and sleep consistency.
- Multiple Sleep Latency Test (MSLT): Measures how quickly you fall asleep during scheduled daytime naps, used to diagnose narcolepsy or assess the severity of daytime sleepiness.
- Sleep diary: A low‑tech but essential tool that captures patterns in sleep timing, duration, quality, and daytime symptoms over time.
- Blood work or medical review: Checks for thyroid imbalances, iron deficiency (linked to restless legs), medication side effects, or hormonal changes like menopause.
Red‑flag criteria that warrant sleep testing include loud snoring with witnessed breathing pauses, excessive daytime sleepiness that affects safety (like dozing while driving), symptoms occurring three or more nights per week for three months or longer, and reliance on alcohol or sleep medications just to fall asleep.
Evidence‑Based Treatments That Improve Restorative Sleep
Cognitive Behavioral Therapy for Insomnia (CBT‑I) is the first‑line treatment for chronic insomnia and has strong evidence for improving both sleep quality and daytime functioning. It’s a structured, skills‑based approach that addresses the thoughts, behaviors, and patterns keeping you awake or stuck in light sleep. CBT‑I typically includes sleep restriction (temporarily limiting time in bed to consolidate sleep), stimulus control (re‑associating the bed with sleep instead of wakefulness), and cognitive techniques to manage racing thoughts and sleep‑related anxiety. Improvements often show up over several weeks, and the skills stick long‑term.
For obstructive sleep apnea, treatment usually involves a breathing device like CPAP (continuous positive airway pressure), which keeps the airway open during sleep and eliminates the repeated awakenings caused by pauses in breathing. Most people notice a significant improvement in morning refreshment and daytime energy once apnea is treated, though it can take a few weeks to adjust to wearing the device. Restless legs syndrome and periodic limb movements may require a medical review to check iron levels, adjust medications that worsen symptoms, or try targeted therapies when appropriate.
Sleep medications and over‑the‑counter supplements like melatonin can play a short‑term role, but they come with trade‑offs. Next‑day grogginess, tolerance over time, risk of masking an underlying disorder, potential interactions with other medications. Any use should be discussed with a clinician, ideally as part of a broader treatment plan that includes behavioral and environmental changes.
Practical at‑home steps that directly support restorative sleep:
- Keep a consistent wake time every day, even on weekends, to stabilize your circadian rhythm.
- Dim lights one to two hours before bed to support natural melatonin release.
- Create a short, predictable wind‑down routine. Slow breathing, light stretching, reading, or a warm shower.
- Keep your bedroom cool (around 65–68°F if possible), dark, and as quiet as you can manage.
- Move caffeine cutoff to early afternoon and limit alcohol close to bedtime.
- Get regular physical activity, but avoid intense workouts within two to three hours of sleep.
When Morning Exhaustion Needs Medical Evaluation
Morning exhaustion that shows up a few times after a stressful week or a late night is normal. Morning exhaustion that happens most days, despite spending enough time in bed and trying basic sleep hygiene, is not. It’s worth reaching out to a clinician when your sleep problems meet certain thresholds: occurring three or more nights per week, lasting three months or longer, causing noticeable impairment in your work, mood, or daily life.
You should seek evaluation sooner if you notice safety concerns. Dozing off while driving, operating machinery, or in situations where a lapse in attention could be dangerous. Loud snoring, gasping, choking sounds, or witnessed pauses in breathing are red flags for obstructive sleep apnea and warrant prompt testing. If you’re relying on alcohol, sleep medications, or over‑the‑counter aids just to fall asleep, that’s another sign the underlying problem needs attention rather than temporary management.
High‑priority signs that warrant clinical review:
- Loud snoring with witnessed breathing pauses or gasping during sleep.
- Excessive daytime sleepiness that impairs safety, especially while driving or during passive activities.
- Symptoms occurring three or more nights per week for three months or longer, with clear daytime consequences.
- Dependence on alcohol, prescription sleep aids, or over‑the‑counter medications to fall or stay asleep.
Final Words
You wake up after 7–9 hours and still feel heavy, foggy, and slow to move. We defined non‑restorative sleep, showed how fragmented sleep and lost deep sleep leave you unrefreshed, and listed the key signs to notice.
You also saw common medical causes, lifestyle triggers, diagnostic tools, and treatments—plus simple at‑home steps and tracking to bring to a clinician.
If this sounds familiar, start tracking and try small, safe changes. non-restorative sleep and morning exhaustion what it means is often manageable, and there are clear next steps to feel better.
FAQ
Q: What does it mean to have non-restorative sleep?
A: Having non-restorative sleep means waking unrefreshed despite enough time in bed (usually 7–9 hours), often from fragmented sleep, micro-awakenings, or loss of deep and REM sleep stages.
Q: Does sleep affect A1c levels?
A: Sleep affects A1c levels because poor or short sleep can raise average blood sugar over time, increasing A1c; improving sleep often helps glucose control but doesn’t replace medical care.
Q: What causes lack of restorative sleep?
A: Lack of restorative sleep is caused by sleep fragmentation, sleep disorders like apnea or restless legs, chronic pain, late caffeine or alcohol, inconsistent schedules, stress, or poor bedroom conditions.
Q: What does unrefreshing sleep feel like?
A: Unrefreshing sleep feels like waking groggy and heavy-headed, with brain fog, morning exhaustion, headaches, slowed thinking, or ongoing tiredness even after a full night’s sleep.
Comments are closed