
Tired of feeling like your belly is a balloon most days?
Constant bloating and indigestion are common, but they aren’t things you should have every day.
When they stick around, they often point to patterns in how your gut moves, what you eat, gut bacteria, or how your nervous system sends pain signals.
This post explains the likeliest medical causes—IBS, food intolerances (lactose, gluten, high-FODMAPs), constipation, acid reflux, and SIBO—and how each one produces persistent symptoms.
You’ll get simple, low-risk steps to try, what to track, and when to seek medical care.
Key Medical Reasons Behind Constant Bloating and Indigestion
Bloating and indigestion feel uncomfortable in different ways, but they often show up together. Bloating is that stretched, full sensation, like a balloon in your belly. Sometimes with visible swelling, belching, or the urge to pass gas. Indigestion (also called dyspepsia) is upper stomach discomfort that can include burning, nausea, early fullness during a meal, or a gnawing ache. When either one happens occasionally after a big meal or a stressful day, that’s normal. When they happen most days or stick around for weeks, something else is going on in your digestive system.
Nearly 1 in 7 people in the United States report bloating at least once a week, and many describe it as constant. That figure comes from survey data including 88,795 Americans, so you’re definitely not alone. The gastrointestinal tract is sensitive. Persistent symptoms usually point to an underlying pattern, not a single bad meal. Most causes fall into a few clear categories: how your gut moves food along, what you’re eating, how your gut bacteria behave, and how your nervous system interprets signals from your abdomen.
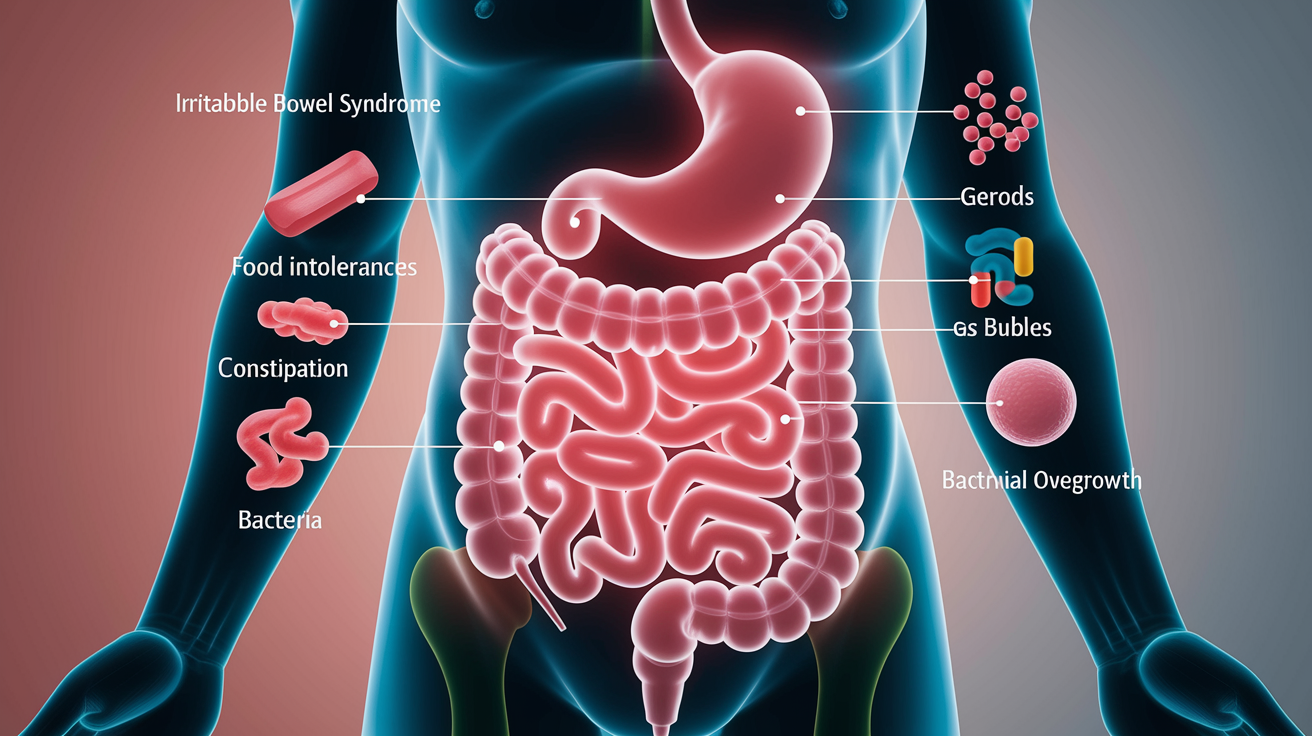
The most common medical explanations for ongoing bloating and indigestion include irritable bowel syndrome, food intolerances, constipation, acid reflux, and small intestinal bacterial overgrowth. Each one creates symptoms in a slightly different way. Many people deal with more than one at the same time. Understanding which pattern fits your experience makes it easier to narrow down next steps.
The top cause categories are:
Irritable bowel syndrome (IBS): a functional disorder marked by abdominal pain, bloating, and changes in bowel habits (diarrhea, constipation, or both).
Food intolerances: lactose, gluten, and high-FODMAP foods that ferment in the gut and produce excess gas.
Constipation: slow transit gives bacteria more time to create gas, leading to trapped air and abdominal discomfort.
Gastroesophageal reflux disease (GERD): stomach acid backing up into the esophagus, often accompanied by upper belly fullness and burning.
Small intestinal bacterial overgrowth (SIBO): too many bacteria in the small intestine, causing malabsorption, gas, and bloating after meals.
Food Intolerances and Their Role in Ongoing Bloating and Indigestion
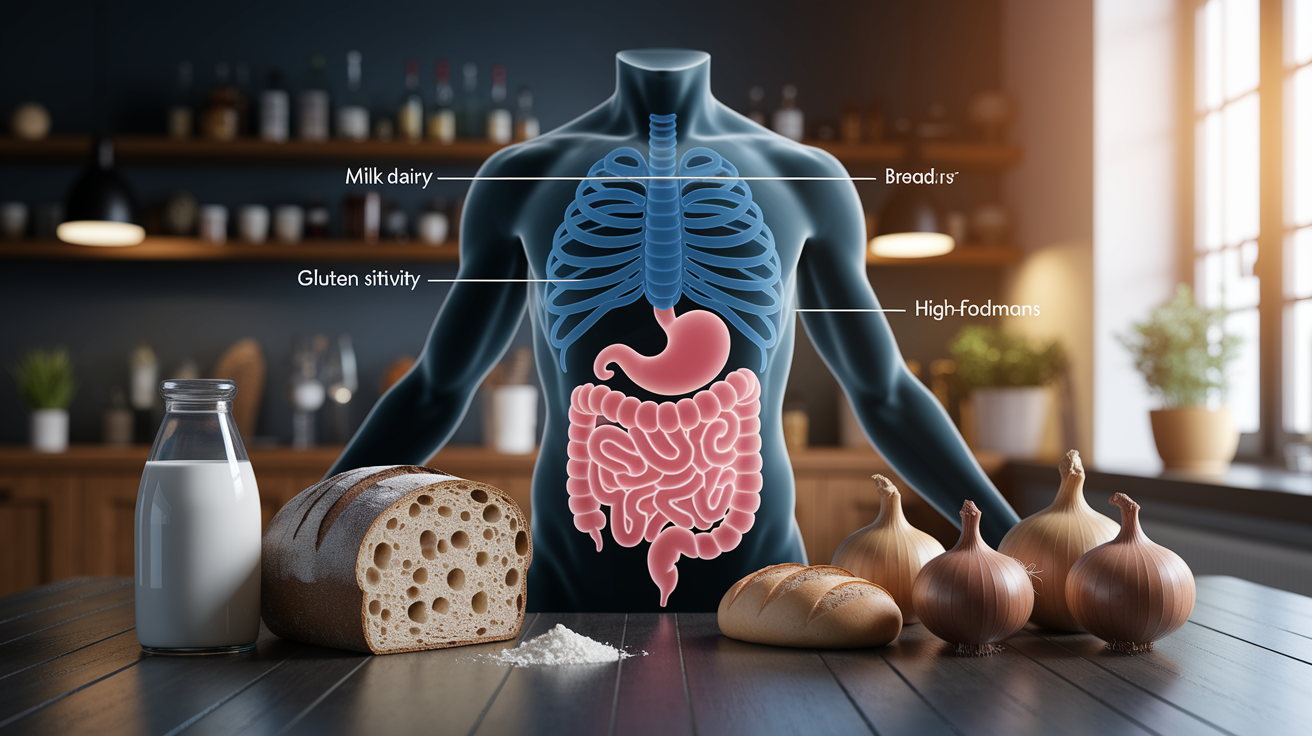
Food intolerances are one of the most common reasons bloating and indigestion happen day after day. Unlike a food allergy, which involves your immune system and can cause hives or breathing trouble, an intolerance means your digestive system struggles to break down a specific component in food. The undigested pieces travel to your colon, where bacteria ferment them and produce gas. That fermentation process creates the tight, swollen feeling and the urge to belch or pass gas.
Three intolerances stand out because they’re widespread and often overlooked: lactose (the sugar in dairy), gluten (a protein in wheat and related grains), and high-FODMAP carbohydrates (a group of short-chain sugars and fibers that ferment quickly). Each one has a slightly different symptom pattern, but all of them can cause daily bloating and indigestion if you keep eating the trigger food without realizing it’s the problem.
Lactose Intolerance
Lactose intolerance happens when your small intestine doesn’t make enough lactase, the enzyme that breaks down milk sugar. Without it, lactose moves into your colon undigested, and bacteria go to work on it, producing hydrogen gas and sometimes methane. That gas buildup causes bloating, cramping, rumbling, and often diarrhea within 30 minutes to two hours after eating dairy.
Common clues: symptoms show up after milk, cheese, yogurt, ice cream, or cream-based sauces, but not after lactose-free dairy or hard aged cheeses (which contain less lactose). Many people notice the pattern only after they try cutting dairy for a few days and feel noticeably better. Over-the-counter lactase enzyme pills, like Lactaid, can reduce symptoms if you take them right before eating dairy.
Gluten Sensitivity
About 6 percent of people in the United States have non-celiac gluten sensitivity, which means gluten triggers digestive and systemic symptoms even though they don’t have celiac disease. The typical gut complaints include bloating, gas, abdominal pain, and diarrhea after eating bread, pasta, baked goods, or anything made with wheat, barley, or rye. But gluten sensitivity also causes symptoms outside the digestive system. Headaches, brain fog, joint pain, fatigue, and sometimes a red, itchy rash.
Because the symptoms are so varied, many people don’t connect them to gluten until they eliminate it for two or three weeks and see improvement. If you suspect gluten, it’s worth getting tested for celiac disease before you stop eating it, because the antibody tests only work if gluten is still in your diet.
High-FODMAP Triggers
FODMAPs are fermentable oligosaccharides, disaccharides, monosaccharides, and polyols. Basically, a collection of short-chain carbohydrates and sugar alcohols that pull water into your intestines and ferment quickly in the colon. High-FODMAP foods include beans, lentils, onions, garlic, apples, pears, stone fruits, cauliflower, mushrooms, and sugar-free sweeteners like sorbitol and xylitol.
When you eat several high-FODMAP foods in one day, the fermentation can be intense, producing large amounts of gas and causing visible abdominal distension. Many people describe it as feeling “pregnant” by evening even though their stomach was flat in the morning. A low-FODMAP elimination diet, done with guidance from a dietitian, can help you identify which specific foods are your main triggers.
Intolerance-related bloating usually follows a clear timing pattern. It gets worse within a few hours of eating the trigger food and may last into the next morning. That’s different from IBS bloating, which can fluctuate with stress, or constipation bloating, which builds gradually over days.
How Constipation Causes Repeated Bloating and Indigestion
Constipation is one of the most underrecognized causes of daily bloating and indigestion. When stool moves slowly through your colon, it sits there longer, giving bacteria extra time to ferment whatever’s left over from digestion. That fermentation produces methane and hydrogen gas, which get trapped behind the backed-up stool and cause pressure, cramping, and visible distension. The longer things stay stuck, the worse the bloating gets.
Common signs of constipation include fewer than three bowel movements per week, hard or lumpy stools (like pebbles or logs with cracks), straining, a feeling that you can’t fully empty your bowels, and sometimes a dull ache low in your abdomen or back. You might also notice bloating that feels worse in the evening and better after a bowel movement. Some people see streaks of bright red blood on the toilet paper from straining, which usually signals a small tear (fissure) or hemorrhoid rather than something serious, but it’s still worth mentioning to a clinician if it keeps happening.
Simple steps that often help with constipation-related bloating:
Increase fiber gradually: add whole grains, beans, fruits with skin, vegetables, and nuts, but do it slowly over a week or two to avoid making gas worse.
Drink more water: aim for at least 8 cups a day, more if you’re active or it’s hot. Fiber needs water to work properly.
Move your body: even a 10 or 15 minute walk after meals can help stimulate your intestines and move things along.
Pay attention to timing: try to use the bathroom around the same time each day, ideally after breakfast or coffee, when your colon is naturally more active.
Digestive Disorders Like IBS and Their Link to Constant Bloating and Indigestion
Irritable bowel syndrome is one of the most common reasons people experience chronic bloating and indigestion together. IBS is a functional disorder, which means your gut looks normal on tests but doesn’t work the way it should. The hallmark features are abdominal pain that improves after a bowel movement, plus changes in how often or how easily you go. Diarrhea, constipation, or a mix of both. Bloating and gas are almost always part of the picture. Many people say the bloating is the most bothersome symptom of all.
IBS Symptom Patterns
IBS symptoms tend to follow predictable triggers. They often get worse after eating, especially large meals or foods high in fat or FODMAPs. Stress, lack of sleep, and hormonal shifts (like the week before your period) can also ramp up cramping and bloating. Some people notice their symptoms flare during busy or emotionally difficult weeks, then calm down on vacation or during quieter stretches. The pain usually comes in waves or cramps, often in the lower belly, and it might shift locations from one day to the next.
Bowel habit changes are a key part of the diagnosis. IBS-D (diarrhea-predominant) means loose or urgent stools most of the time. IBS-C (constipation-predominant) means hard, infrequent stools. IBS-M (mixed) means you alternate between the two, sometimes within the same week. Bloating can happen with any subtype, but it tends to be most severe with IBS-C because of the gas buildup behind slow-moving stool.
Visceral Hypersensitivity
One reason IBS causes so much discomfort is visceral hypersensitivity. Your gut nerves send stronger pain signals to your brain than they should. A normal amount of gas or stretch in your intestines, which most people wouldn’t notice, feels painful or intensely uncomfortable when you have IBS. It’s not that you’re imagining the pain. Your nervous system is genuinely more reactive. That heightened sensitivity is also why stress, anxiety, and lack of sleep make IBS symptoms worse. Your brain and gut are in constant two-way communication, and when one is on edge, the other follows.
IBS doesn’t have a single cause or a one-size-fits-all cure, which is why management is tailored to each person. Most treatment plans combine dietary changes (often a low-FODMAP trial), stress management, regular sleep and exercise, and sometimes medications to regulate bowel movements or reduce pain. Early diagnosis and a clear plan can prevent symptoms from getting worse and help you feel more in control of day-to-day life.
Small Intestinal Bacterial Overgrowth (SIBO) and Ongoing Digestive Discomfort

Small intestinal bacterial overgrowth happens when bacteria that normally live in your colon migrate up into your small intestine and start multiplying there. Your small intestine is supposed to have relatively few bacteria because that’s where most nutrient absorption happens. When too many bacteria set up shop, they ferment food before your body can absorb it properly, producing large amounts of gas (often hydrogen, methane, or both) and causing malabsorption, bloating, abdominal pain, and changes in your stool.
SIBO often feels similar to IBS, which is why it sometimes goes undiagnosed for years. The main difference is timing: SIBO bloating and discomfort usually start within 30 to 60 minutes after eating, especially after meals with carbohydrates or fiber, because that’s what the bacteria love to ferment. You might also notice weight loss, nutrient deficiencies (like low iron or B12), or greasy, foul-smelling stools if fat absorption is affected.
| Cause | Effect in Digestion |
|---|---|
| Malabsorption | Bacteria consume nutrients before your body can absorb them, leading to deficiencies and weight loss. |
| Excess gas production | Fermentation of carbohydrates and fiber creates large volumes of hydrogen and methane, causing bloating and distension. |
| Slowed motility | Conditions that slow gut movement (like diabetes, scleroderma, or prior surgery) allow bacteria to overgrow and stay in the small intestine. |
Contributing factors for SIBO include motility disorders that slow the normal sweeping action of your intestines, structural abnormalities from surgery or strictures, inflammatory bowel disease, and long-term use of medications that reduce stomach acid (like proton pump inhibitors). Diagnosis usually involves a breath test that measures hydrogen and methane levels after you drink a sugar solution. Treatment typically includes a course of antibiotics, followed by dietary adjustments and sometimes a prokinetic medication to help your gut move food along more efficiently.
Motility Disorders and Slow Digestion in Chronic Bloating and Indigestion

Motility disorders are conditions where the muscles and nerves in your digestive system don’t coordinate properly, so food and gas move too slowly, or sometimes not at all. That sluggish transit gives bacteria more time to ferment everything, which means more gas production, more bloating, and often a heavy, uncomfortable fullness that lasts for hours after eating. Gastroparesis is one of the most common motility problems. It means your stomach empties too slowly, so food sits there longer than it should, causing nausea, early fullness, bloating, and sometimes vomiting of undigested food.
Gastroparesis can be caused by diabetes (high blood sugar damages the vagus nerve that controls stomach contractions), prior abdominal surgery, certain medications, or autoimmune conditions. Other motility disorders affect the small intestine or colon and can be linked to connective tissue diseases like scleroderma, neurological conditions, or simply idiopathic (no clear cause found). Clues that point toward a motility problem include bloating and nausea that are worst after meals, vomiting several hours after eating, feeling full after just a few bites, and weight loss because eating becomes so uncomfortable you start avoiding food.
Diagnosis often involves imaging tests like a gastric emptying scan, where you eat a small radioactive meal and a scanner tracks how long it takes to leave your stomach, or motility studies that measure pressure and movement throughout your digestive tract. Treatment focuses on smaller, more frequent meals, foods that are easier to digest (less fat and fiber during flares), medications that help the stomach contract (prokinetics), and sometimes treatments to manage nausea. In severe cases, feeding tubes or surgical options may be needed, but most people manage well with dietary and medication adjustments.
Hormonal Changes and Their Contribution to Indigestion and Bloating
Hormonal fluctuations, especially around your menstrual cycle and during perimenopause, are a well-known trigger for bloating and indigestion. Many people notice their belly feels tighter and more distended in the week before their period, even if their eating habits haven’t changed. That cyclical bloating is driven by shifts in estrogen and progesterone, which affect how much water your body retains, how quickly food moves through your gut, and how sensitive your intestines are to gas and stretch.
Progesterone, which rises after ovulation, relaxes smooth muscle tissue throughout your body, including the muscles in your digestive tract. That can slow down motility and make you more prone to constipation and trapped gas. At the same time, changing hormone levels can increase inflammation and fluid retention, which adds to the swollen, uncomfortable feeling. Some people also experience increased appetite, cravings for salty or sweet foods, mood changes, and fatigue, all of which can influence eating patterns and digestion during that premenstrual window.
Typical patterns and relief strategies:
Timing: bloating usually starts a few days to a week before your period and improves once bleeding begins or shortly after.
Accompanying symptoms: breast tenderness, mood swings, headaches, lower back ache, and cravings often cluster together with the bloating.
Simple relief: reduce salt intake, stay well hydrated (aim for 48 to 64 ounces of water daily), avoid alcohol, and try gentle movement like walking or yoga to ease fluid retention and support gut motility.
Eating Habits and Lifestyle Behaviors That Trigger Ongoing Indigestion and Bloating

Even when there’s no underlying medical condition, certain everyday habits can cause bloating and indigestion that feel just as uncomfortable and persistent. Swallowed air is one of the biggest culprits, and most of us do it without realizing. Every time you chew gum, suck on hard candy, drink through a straw, gulp down a meal in five minutes, or talk while eating, you swallow small pockets of air. That air has to go somewhere, either up as a belch or down through your intestines as gas.
Eating large meals all at once, rather than smaller portions spread throughout the day, also overwhelms your digestive system. Your stomach and intestines have to work harder and longer to break everything down, which increases the chance of fermentation, reflux, and that heavy, sluggish feeling. Carbonated beverages add even more gas directly into your stomach. If you’re already dealing with slow motility or a sensitive gut, that extra carbonation can tip you into visible bloating and discomfort.
Common behaviors that increase bloating and indigestion:
Chewing gum or sucking on hard candies: you swallow air with every chew or suck, plus many sugar-free versions contain sorbitol or xylitol, which are high-FODMAP and ferment in your colon.
Eating too quickly: when you rush, you don’t chew thoroughly, so larger food particles reach your intestines and bacteria have to do more work, producing more gas.
Drinking through a straw: each sip pulls in a little extra air.
Large meals: your stomach stretches, digestion slows, and fermentation increases.
Carbonated drinks: soda, sparkling water, and beer release carbon dioxide in your stomach, adding to bloating.
Talking while eating: you swallow air along with your food.
Lying down right after eating: gravity helps keep stomach contents down. Lying flat can worsen reflux and make bloating feel more intense.
Small changes make a real difference. Eat slowly, put your fork down between bites, chew each mouthful thoroughly, avoid gum and hard candies, skip the straw, and stay upright for at least an hour after meals. If carbonated drinks are part of your daily routine, try cutting them out for a week and see if your bloating improves. You might be surprised by how much lighter you feel.
More Serious Conditions That Can Cause Constant Bloating and Indigestion

Most chronic bloating and indigestion come from functional issues like IBS, food intolerances, or constipation, but a smaller percentage of cases are caused by structural or inflammatory diseases that need medical diagnosis and treatment. These conditions often come with additional red-flag symptoms. Unintended weight loss, blood in your stool, persistent vomiting, severe pain, or systemic signs like fever, fatigue, or night sweats. If you’re experiencing any of those alongside daily bloating, it’s time to see a clinician for a full workup.
Celiac disease, inflammatory bowel disease (Crohn’s disease and ulcerative colitis), gallbladder problems, pancreatic insufficiency, and liver disease can all cause chronic bloating and indigestion. Each one has its own diagnostic signature, but they share the feature of causing damage or dysfunction that shows up on lab tests, imaging, or endoscopy. That’s different from IBS or food intolerances, which are diagnosed by symptoms and pattern recognition rather than abnormal test results.
Catching these conditions early matters. Untreated celiac disease damages your small intestine and increases the risk of nutrient deficiencies, osteoporosis, and other autoimmune diseases. Inflammatory bowel disease can lead to strictures, fistulas, and an increased risk of colon cancer if it’s not managed. Gallbladder disease and pancreatic insufficiency interfere with fat digestion and absorption, causing deficiencies in fat-soluble vitamins. Liver disease can progress to cirrhosis and life-threatening complications. Early diagnosis and appropriate treatment prevent those outcomes and improve quality of life.
| Condition | Key Symptoms | Typical Clues |
|---|---|---|
| Celiac disease | Chronic diarrhea, bloating, weight loss, fatigue, anemia | Symptoms improve on a strict gluten-free diet; positive blood antibodies and small-intestine biopsy confirm diagnosis |
| Inflammatory bowel disease (Crohn’s or ulcerative colitis) | Bloody diarrhea, abdominal pain, weight loss, fever, joint pain | Visible inflammation or ulcers on colonoscopy; elevated inflammatory markers in blood and stool |
| Gallbladder problems (stones or dysfunction) | Right upper belly pain after fatty meals, nausea, bloating | Pain may radiate to the back or shoulder; ultrasound shows stones or sludge; abnormal liver enzymes during an attack |
| Pancreatic insufficiency | Greasy, foul-smelling stools, weight loss, bloating, gas | Often linked to chronic pancreatitis or cystic fibrosis; stool tests show high fat content; enzyme supplements improve symptoms |
Diagnostic Tests Used to Uncover Causes of Daily Bloating and Indigestion

When bloating and indigestion are persistent, your clinician will use a combination of your symptom history, physical exam findings, and targeted tests to figure out what’s going on. The first step is usually a detailed conversation about when symptoms started, what makes them better or worse, your bowel habits, your diet, medications, stress levels, and any red-flag signs. That history alone often points toward the most likely category. Functional disorder, food intolerance, motility problem, or something structural.
Lab tests typically include a complete blood count (to check for anemia or infection), liver and kidney function, thyroid levels, and inflammatory markers like C-reactive protein or fecal calprotectin (which are elevated in inflammatory bowel disease but normal in IBS). If celiac disease is suspected, your clinician will order tissue transglutaminase antibodies while you’re still eating gluten. Stool studies can check for infections, blood, fat content, and markers of inflammation.
Common diagnostic tools for persistent bloating and indigestion:
Breath tests: used to diagnose lactose intolerance, fructose malabsorption, and small intestinal bacterial overgrowth (SIBO) by measuring hydrogen and methane levels after you drink a sugar solution.
Upper endoscopy (EGD): a scope passed through your mouth into your esophagus, stomach, and duodenum to look for ulcers, inflammation, celiac damage, or H. pylori infection. Biopsies can be taken during the procedure.
Colonoscopy: a scope inserted through the rectum to examine your colon and the end of your small intestine. Used to diagnose inflammatory bowel disease, polyps, or other structural issues.
Imaging studies: abdominal ultrasound, CT scan, or MRI to visualize your gallbladder, liver, pancreas, and intestines. A gastric emptying scan measures how quickly your stomach empties.
When Constant Bloating and Indigestion Signal the Need for Medical Care
Occasional bloating after a big meal or a stressful week is normal and usually goes away on its own with rest, hydration, and lighter eating. But when bloating and indigestion happen most days, interfere with your ability to work or enjoy life, or come with other worrying symptoms, it’s time to see a clinician. Red-flag symptoms mean something more serious might be going on. Catching it early makes treatment easier and more effective.
Warning signs that you should not wait to address:
Unexplained weight loss: losing 10 pounds or more without trying, especially over a few weeks or months.
Blood in your stool: bright red, dark tarry stools, or a positive fecal occult blood test.
Severe or worsening abdominal pain: pain that wakes you at night, keeps you from eating, or is localized to one spot and getting worse.
Persistent vomiting: especially if you’re vomiting undigested food several hours after eating or can’t keep liquids down.
High fever: a temperature above 101°F along with bloating and abdominal pain.
Inability to pass stool or gas: complete obstruction is a medical emergency and requires immediate evaluation.
Practical Relief Strategies for Constant Bloating and Indigestion
Most chronic bloating and indigestion improve with a combination of dietary adjustments, habit changes, and simple self-care measures. The goal is to reduce the amount of gas your gut produces, help food and gas move through more efficiently, and lower your overall digestive stress. These strategies are low-risk, evidence-informed, and worth trying before or alongside medical treatment.
Start with your eating pace and portion sizes. Eating slowly and chewing each bite thoroughly gives your stomach and enzymes time to start breaking down food properly, which means less fermentation and gas production downstream. Smaller, more frequent meals (say, five or six small portions instead of three large ones) reduce the workload on your digestive system and prevent that overstuffed, sluggish feeling. Staying upright for at least an hour after eating uses gravity to your advantage and can ease both bloating and reflux.
Practical steps to try now:
Eat slowly and chew thoroughly: aim for at least 15 to 20 minutes per meal. Put your fork down between bites.
Limit carbonated drinks: skip soda, sparkling water, and beer for a week and see if bloating decreases.
Stay well hydrated: drink water throughout the day, aiming for at least 8 cups. Proper hydration supports motility and softens stool.
Add light post-meal movement: a 10 minute walk after eating can stimulate gut motility and reduce gas buildup.
Try lactase enzyme before dairy: if you suspect lactose intolerance, take an over-the-counter lactase pill right before eating dairy to see if symptoms improve.
Consider a low-FODMAP trial: work with a dietitian to eliminate high-FODMAP foods for two to six weeks, then systematically reintroduce them to identify your specific triggers.
Tracking your symptoms and what you eat for at least a week or two creates a useful map. Note the time of day, what you ate, portion size, how you felt before and after, your stress level, where you are in your cycle, and your bowel habits. Patterns will start to emerge. Maybe bloating is worse after dairy, or it spikes the week before your period, or it improves on days when you walk after dinner. That information is gold when you sit down with a clinician, because it helps narrow the list of possible causes and makes your treatment plan more precise.
Final Words
If you feel full, gassy, and uncomfortable most days, this post walked through the likely culprits: food intolerances, IBS and SIBO, constipation, slow motility, hormones, eating habits, and less common medical concerns. It also covered common tests and clear red flags.
Start with low-risk steps: slow down while eating, hydrate, try gentle movement, and note what makes symptoms better or worse.
If you’re still asking what causes constant bloating and indigestion, use the tracking tips and bring them to a clinician. Small changes often lead to clearer answers and real relief.
FAQ
Q: Why do I always feel bloated and have indigestion? What does persistent bloating mean?
A: Always feeling bloated with indigestion usually means your gut reacts to a repeated trigger—like food intolerance, IBS, constipation, SIBO, or reflux. Track patterns and seek care for severe or worsening signs.
Q: What are four signs that your digestive system isn’t working properly? What are the 7 signs of indigestion?
A: Key signs your digestive system isn’t working, and common indigestion signs, include bloating, frequent belly pain, heartburn, nausea, persistent diarrhea or constipation, and unexplained weight loss or blood in stool.
Comments are closed